Focused Shockwave Therapy for Gluteal Tendinopathy
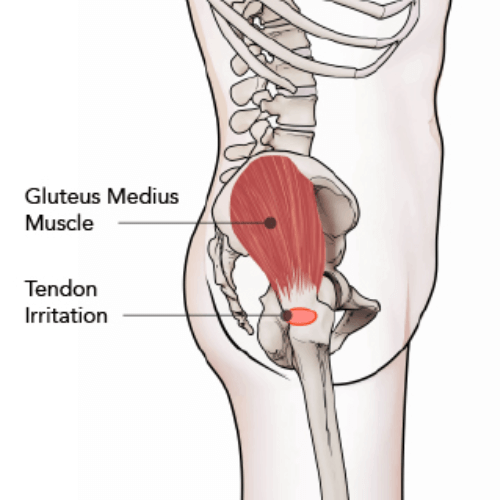
Gluteal tendinopathy is the most common cause of persistent lateral hip pain and involves degeneration or partial tearing of the gluteus medius and/or gluteus minimus tendons at their attachment on the greater trochanter. Often described as the “rotator cuff tear of the hip,” this condition most commonly affects adults between ages 50–70 and occurs more frequently in women.
Current research shows that most lateral hip pain is tendon-related rather than isolated bursitis. True primary bursitis is uncommon, and when bursal irritation is present, it is typically secondary to underlying gluteal tendon dysfunction. The primary mechanical driver is excessive compressive and tensile loading at the tendon insertion, particularly affecting the deeper anterior fibers.
Because gluteal tendinopathy is a degenerative tendon disorder rather than an inflammatory condition, treatment focuses on restoring tendon load capacity and improving hip biomechanics. Focused Shockwave Therapy is a non-invasive treatment that may be incorporated into conservative management when progressive loading exercises alone do not fully resolve symptoms.
Can shockwave therapy help gluteal tendinopathy?
Yes. Extracorporeal shockwave therapy (ESWT), including focused shockwave therapy, has been evaluated in patients with greater trochanteric pain syndrome, a condition frequently driven by gluteal tendon pathology.
Randomized controlled trials report improvements in pain and functional outcomes following shockwave therapy. It is typically considered in chronic cases that have not responded adequately to load-based rehabilitation alone.
Shockwave therapy delivers targeted acoustic energy to degenerative tendon tissue and is integrated into structured rehabilitation rather than used as a standalone intervention.
What is the most effective treatment for gluteal tendinopathy?
Evidence consistently supports education combined with progressive exercise as the foundation of treatment.
Load modification strategies are essential. These include avoiding sustained hip adduction (such as crossing legs or leaning onto one hip), improving gait mechanics, and modifying sleep positioning. Rehabilitation progresses from isometric loading, which may provide short-term pain relief, to eccentric and functional strengthening designed to restore tendon capacity.
Research demonstrates that education combined with exercise provides superior long-term outcomes compared to corticosteroid injections. While injections may provide temporary relief, benefits are often not sustained.
For patients with persistent symptoms despite appropriate loading programs, non-surgical adjuncts such as shockwave therapy may be incorporated.
How many sessions of shockwave therapy are used for gluteal tendinopathy?
Clinical trials studying shockwave therapy for greater trochanteric pain syndrome typically deliver treatment across a short series of sessions spaced over several weeks.
Protocols vary based on device type, energy level, and patient presentation. Treatment plans are individualized following clinical assessment. Shockwave therapy is most effective when combined with progressive strengthening and movement retraining.
Can shockwave therapy help tendinopathy?
Shockwave therapy has been studied across multiple chronic tendinopathies. Clinical research supports its use in select chronic tendon conditions where symptoms persist despite conservative loading programs.
It is considered a non-surgical option that may help improve pain and functional outcomes when integrated into a comprehensive tendon rehabilitation strategy.
At Cole Pain Therapy Group in Memphis, gluteal tendinopathy is evaluated through detailed clinical testing to confirm tendon involvement and identify contributing biomechanical factors. Assessment includes palpation of the greater trochanter, single-leg stance testing, resisted tendon evaluation, and gait analysis to determine whether symptoms are consistent with degenerative gluteal tendon pathology.
When appropriate, treatment focuses on progressive gluteal strengthening, load modification, and movement retraining to restore tendon capacity. For patients with persistent lateral hip pain despite structured rehabilitation, Focused Shockwave Therapy may be incorporated as a non-surgical, tendon-directed intervention to support tissue remodeling and reduce pain. Patients from Memphis, Bartlett, Lakeland, and Arlington seek care when hip pain interferes with walking, stairs, or sleep.
NEW PATIENTS
Step 1
Call today to schedule your convenient appointment.
Step 2
Pre-register your important health information on your phone or computer to save time.
Step 3
Meet your new doctor for a customized plan and start moving toward your goal!
Discover how we may help!
We are the Memphis area’s top-rated chiropractic group, providing you with gentle chiropractic care, dry needle therapy, exercise therapy, and therapeutic massage.

2845 Summer Oaks Dr, Memphis, TN 38134
(901) 377-2340
Life Shouldn't Hurt!
You Deserve To Feel Great. We Can Help!
Your go-to Chiropractor in Memphis, TN
Richard L. Cole, DC, DACNB, DAIPM, FIACN, FICC
Jeffrey D. Luebbe, DC, CCRD, CCSP
W. Steven Vollmer, DC, DAAPM
Bradford J. Cole, DC, MS, CSCS
J. Colby Poston, DC
Daniel H. Smith, DC
2845 Summer Oaks Dr., Memphis, TN 38134
(901) 377-2340
Monday – Friday:
8:00 AM – 6:00 PM
Saturday :
8:00 AM – 12:00 PM
Walk-ins are Welcome!
© 2025 Cole Pain Therapy Group, All Rights Reserved