Focused Shockwave Therapy for Posterior Tibial Tendinopathy
Posterior tibial tendinopathy, also known as posterior tibial tendon dysfunction (PTTD), is the leading cause of adult-acquired flatfoot. The condition typically begins with medial ankle pain and may progress to tendon degeneration and collapse of the medial longitudinal arch if not recognized early. The posterior tibialis muscle functions as the primary dynamic stabilizer of the arch, especially during push-off in walking and running.
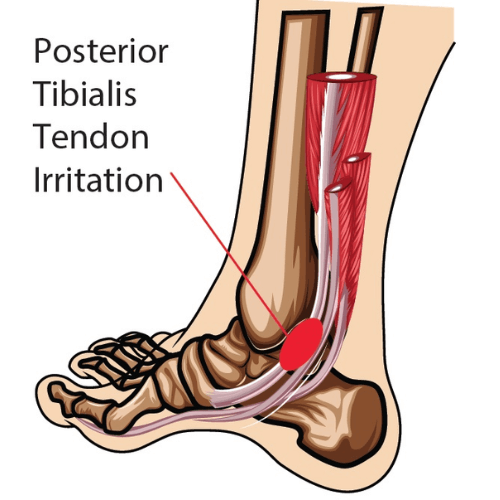
Repetitive strain that exceeds the tendon’s tolerance initiates a progression from irritation to failed healing, fibrosis, and degeneration. The most common site of pathology is a relatively hypovascular region just behind the medial malleolus. Early-stage disease (Stage I and II) remains flexible and is usually appropriate for conservative care, while advanced stages (Stage III and IV) involve rigid deformity, ligament compromise, and potential need for surgical intervention.
Because posterior tibial tendinopathy reflects degenerative tendon pathology rather than persistent inflammation, treatment focuses on restoring tendon capacity, improving mechanical support, and stimulating tissue remodeling. Focused Shockwave Therapy is a non-invasive modality that may be incorporated into conservative management for early-stage degenerative tendon conditions when clinically appropriate.
Can shockwave therapy help posterior tibial tendonitis?
Posterior tibial tendon disorders are primarily degenerative rather than purely inflammatory. Shockwave therapy has demonstrated effectiveness in reducing pain in degenerative tendinopathies and is used clinically as part of structured conservative care.
In early-stage posterior tibial tendinopathy where deformity remains flexible and rupture has not occurred, Focused Shockwave Therapy may be incorporated into a rehabilitation program designed to support tendon remodeling and reduce pain.
What is the treatment for posterior tibial tendon dysfunction?
Treatment depends on disease stage and structural integrity.
Stage I and Stage II posterior tibial tendon dysfunction are typically managed conservatively. Care may include activity modification, mechanical support with orthotics or arch supports, progressive strengthening of the posterior tibialis muscle, eccentric loading programs, and stretching of the gastrocnemius–soleus complex. Temporary immobilization may be recommended when symptoms persist.
If symptoms fail to improve after several weeks of structured conservative care, a walking boot or cast may be required. Advanced disease involving rigid deformity or fixed hindfoot valgus generally requires orthopedic or podiatric referral.
Is shockwave therapy good for tendons?
Shockwave therapy is used in the management of degenerative tendinopathies throughout the body. Research demonstrates that shockwave therapy can reduce tendon-related pain and stimulate biological processes associated with tissue repair and collagen remodeling.
It is most effective when integrated into a comprehensive rehabilitation strategy that includes progressive strengthening and mechanical correction rather than used as a standalone intervention.
When should you not use shockwave therapy?
Shockwave therapy is not appropriate in cases involving complete tendon rupture, rigid deformity (Stage III or IV posterior tibial tendon dysfunction), or when surgical reconstruction is indicated.
Advanced disease characterized by fixed hindfoot valgus, ligament failure, or structural collapse requires referral rather than conservative-only management. A thorough clinical evaluation is necessary to determine whether nonoperative care is appropriate.
Shockwave therapy is not appropriate in cases involving complete tendon rupture, rigid deformity (Stage III or IV posterior tibial tendon dysfunction), or when surgical reconstruction is indicated.
Advanced disease characterized by fixed hindfoot valgus, ligament failure, or structural collapse requires referral rather than conservative-only management. A thorough clinical evaluation is necessary to determine whether nonoperative care is appropriate.
At Cole Pain Therapy Group in Memphis, posterior tibial tendinopathy is evaluated through detailed clinical staging, gait assessment, and examination of tendon integrity and arch stability. The goal is to determine whether the condition remains flexible and appropriate for conservative management.
For early-stage degenerative tendon pathology, care programs focus on progressive posterior tibialis strengthening, mechanical support strategies, movement retraining, and when indicated, integration of Focused Shockwave Therapy to support biological remodeling of the tendon.
Patients from Memphis, Bartlett, Lakeland, and Arlington seek care when medial ankle pain interferes with walking, exercise, or daily function. Early intervention is essential to reduce tendon-related pain, prevent arch collapse, and avoid progression to rigid deformity or surgical referral.
If you are experiencing medial ankle pain, swelling behind the medial malleolus, difficulty performing a single-leg heel rise, or progressive flattening of the arch, an evaluation can determine whether you are a candidate for conservative treatment that includes Focused Shockwave Therapy.
NEW PATIENTS
Step 1
Call today to schedule your convenient appointment.
Step 2
Pre-register your important health information on your phone or computer to save time.
Step 3
Meet your new doctor for a customized plan and start moving toward your goal!
Discover how we may help!
We are the Memphis area’s top-rated chiropractic group, providing you with gentle chiropractic care, dry needle therapy, exercise therapy, and therapeutic massage.

2845 Summer Oaks Dr, Memphis, TN 38134
(901) 377-2340
Life Shouldn't Hurt!
You Deserve To Feel Great. We Can Help!
Your go-to Chiropractor in Memphis, TN
Richard L. Cole, DC, DACNB, DAIPM, FIACN, FICC
Jeffrey D. Luebbe, DC, CCRD, CCSP
W. Steven Vollmer, DC, DAAPM
Bradford J. Cole, DC, MS, CSCS
J. Colby Poston, DC
Daniel H. Smith, DC
2845 Summer Oaks Dr., Memphis, TN 38134
(901) 377-2340
Monday – Friday:
8:00 AM – 6:00 PM
Saturday :
8:00 AM – 12:00 PM
Walk-ins are Welcome!
© 2025 Cole Pain Therapy Group, All Rights Reserved