How to Fix Scapular Dyskinesis and Restore Shoulder Function
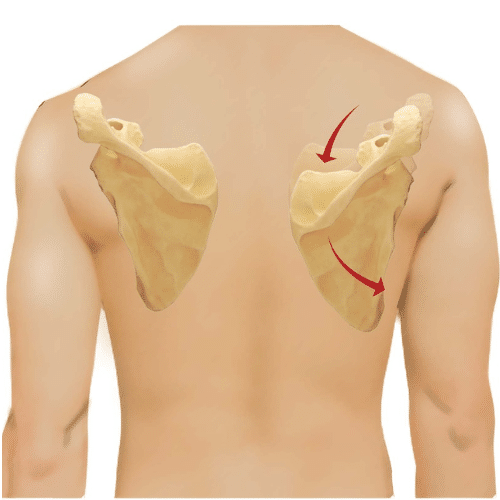
Scapular dyskinesis means the shoulder blade (scapula) isn’t moving or sitting quite right on your ribcage. The shoulder blade and upper-arm bone should move together in a smooth rhythm. When this rhythm is “off,” the rotator cuff and shoulder joint work harder, which can lead to pain, pinching (impingement), and even rotator cuff problems over time.
It’s common in people who use their arms overhead (throwing, swimming, pickleball, painting) and can show up more often on the dominant side.
Why does it happen?
Scapular dyskinesis usually comes from a mix of muscle imbalance and posture:
Tight muscles in the front of the shoulder (often the pectoralis minor and short head of the biceps) pull the shoulder blade forward and down.
Weak or tired muscles in the back (especially serratus anterior and lower/middle trapezius) can’t hold the shoulder blade in a good position.
Posture factors like rounded shoulders, upper-back stiffness, or long hours on a phone or laptop contribute.
Kinetic-chain links: hip abductor or core weakness, Leg Length Discrepancy, foot over-pronation, and even Dysfunctional Breathing patterns can feed into shoulder mechanics.
Nerve issues (less common): irritation of the long thoracic, spinal accessory, or suprascapular nerves can affect the muscles that position the shoulder blade. After a shoulder injury (e.g., Glenohumeral Dislocation), Axillary Neuropathy may also alter shoulder control.
Related shoulder conditions: AC joint irritation, SLAP Lesion, instability, biceps tendon pain, or Frozen Shoulder (Adhesive Capsulitis) may coexist or follow long-standing dyskinesis.
In overhead athletes, limited internal rotation of the shoulder (called Glenohumeral Internal Rotation Deficit—GIRD) often pairs with dyskinesis.
Common symptoms
Scapular dyskinesis can be silent at first. When symptoms show up, people often notice:
Achy pain at the front or top/back of the shoulder
Pinching with overhead motion or during the lowering phase of an arm raise
A sense of weakness, shakiness, or fatigue with repeated lifts/throws
A visible “winging” or asymmetry of the shoulder blades, especially during arm motion
Tender spots over the front of the shoulder (near the coracoid) or the outer top of the shoulder
How we diagnose it
No special scan is required—this is a clinical diagnosis. Your clinician will:
Watch your movement (flexion/abduction with light weights) and the lowering phase, where issues often appear.
Check posture, ribcage and thoracic mobility, and core/hip control.
Look for strength/tightness patterns (tight pecs; weak serratus/lower trap).
Use quick “assist” tests:
Scapular Assistance Test: the clinician helps the blade rotate upward—less pain = muscle imbalance.
Scapular Retraction/Repositioning Tests: holding the blade back and down—better strength/less pain = positive.
If your story suggests other problems (e.g., labral tears, severe instability, or neck referral), imaging may be used to rule those out—not to diagnose dyskinesis itself.
Treatment: simple steps that work
Most people improve with conservative care. The key is addressing all contributors—front-of-shoulder tightness, back-of-shoulder weakness, posture, and the kinetic chain.
1) Calm tight tissues
Myofascial release & stretching for pec minor, biceps, and the back of the shoulder/capsule.
Posterior capsule and pec minor stretches (doorway stretch, sleeper stretch, cross-body reach).
2) Build smart strength (quality over quantity)
Focus on serratus anterior, lower/middle trapezius, and rotator cuff—while keeping the shoulder blade gently retracted and posteriorly tilted (avoid shrugging).
Early activation / low load
Scapular clocks and wall slides
Serratus punches (supine or wall)
Quadruped rock-backs with protraction
Progressions
Low row / “inferior glide” drills
Prone Y (lower trap), T (middle trap), and extension
Push-up plus (on wall, then counter, then floor)
Half-supine pull-up with straps or bands
Overhead athletes / GIRD
Add posterior capsule work and controlled external rotation eccentrics.
Gradually reintroduce throwing/serving mechanics.
3) Posture & spine/chain care
Thoracic mobility (foam roller, open-book rotations).
Address core and hip abductor strength—if these are weak, fix them early.
Consider foot mechanics; orthotics may help if over-pronation or Leg Length Discrepancy is meaningful.
If neck/upper-back stiffness contributes (e.g., Thoracic Segmental Joint Dysfunction), manual therapy/manipulation can improve comfort and muscle activation.
4) Helpful adjuncts
Elastic therapeutic taping (short-term cueing for blade position).
Manual therapy to restore rib, clavicle, and scapulothoracic glide.
Clear load management: reduce provocative overhead volume, then build back gradually.
Most people feel better within 6–12 weeks with consistent home exercise and smart progressions.
When to seek further evaluation
Night pain, true weakness that’s not improving, or a traumatic event
Signs of nerve involvement (progressive winging, marked fatigue, numbness)
Failure to improve after a dedicated 8–12-week rehab plan
Scapular dyskinesis can place extra stress on the shoulder, but it responds well to the right care. By restoring muscle balance, improving posture, and addressing related areas like the spine and hips, most people see relief and better shoulder function within a few weeks to months. Early attention and consistent rehab make the best long-term results.
NEW PATIENTS
Step 1
Call today to schedule your convenient appointment.
Step 2
Pre-register your important health information on your phone or computer to save time.
Step 3
Meet your new doctor for a customized plan and start moving toward your goal!
Discover how we may help!
We are the Memphis area’s top-rated chiropractic group, providing you with gentle chiropractic care, dry needle therapy, exercise therapy, and therapeutic massage.

2845 Summer Oaks Dr, Memphis, TN 38134
(901) 377-2340
Life Shouldn't Hurt!
You Deserve To Feel Great. We Can Help!
Your go-to Chiropractor in Memphis, TN
Richard L. Cole, DC, DACNB, DAIPM, FIACN, FICC
Jeffrey D. Luebbe, DC, CCRD, CCSP
W. Steven Vollmer, DC, DAAPM
Bradford J. Cole, DC, MS, CSCS
J. Colby Poston, DC
Daniel H. Smith, DC
2845 Summer Oaks Dr., Memphis, TN 38134
(901) 377-2340
Monday – Friday:
8:00 AM – 6:00 PM
Saturday :
8:00 AM – 12:00 PM
Walk-ins are Welcome!
© 2025 Cole Pain Therapy Group, All Rights Reserved